
Multiple sclerosis (MS) is a chronic (long-term) disease that affects the central nervous system.
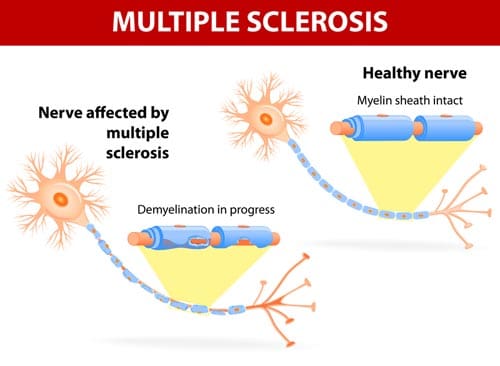
In MS, the protective sheath (known as myelin) that surrounds the nerve fibres in the brain and spinal cord becomes damaged. Myelin acts as an insulator for the nerves, providing protection and helping electrical signals travel from one nerve to the next around the body. Damage to the myelin sheath causes scar tissue to form, leaving hardened (sclerotic) patches — which is how the disease gets its name.
Damage to the myelin disrupts the electrical signals that are normally sent along the nerves. Signals may be slowed or blocked. This is just what happens when the insulating material surrounding an electrical wire is damaged – the electrical signals are no longer transmitted properly through the wire.
It is estimated that over 23,000 Australians currently have MS. MS is not contagious, and most people with the disease are able to live active and productive lives.
What are the symptoms of multiple sclerosis?
The symptoms of MS can vary from person to person and will generally depend on which nerves are affected. Most people only have some of the symptoms listed below.
For example, if MS affects the optic nerve in the eye, a person’s eyesight can be affected. If it affects the nerves in the legs, it may cause difficulty walking.
The most common symptoms of MS include:
- Fatigue
- Weakness, numbness, tingling or painful sensations in the limbs; this usually affects one side of the body at a time, or both legs and the trunk
- Problems with vision, usually in one eye at a time; sometimes eye movements may be painful or a person may have persistent double vision
- Loss of balance, lack of coordination and tremors
- Muscle stiffness or spasms
- Mobility problems
- Bladder, bowel or sexual problems
- Thinking and memory problems
- Depression and anxiety
- Speech and swallowing problems.
The symptoms are often triggered or made worse by an increase in body temperature.
What causes MS?
The exact cause of MS is unknown. MS is a type of auto-immune disease, which means that the body’s immune system mistakenly attacks its own healthy tissue – in this case, myelin. Most experts think that a combination of genetic and environmental factors are involved in the development of MS.
Other factors that may be involved include:
- Viruses: A number of viruses may trigger the development of MS, including Epstein-Barr virus, the virus that causes glandular fever (infectious mononucleosis).
- Lack of sunlight and vitamin D: MS is more common in people who live farthest away for the equator. For example, in Australia, MS is much more common in Tasmania than in more northern states such as Queensland. This suggests that a lack of sunlight (the body’s source of vitamin D) may somehow act as a trigger.
- Smoking: people who smoke are around twice as likely to develop MS compared with people who don’t smoke.
Who gets MS?
MS can occur at any age, but the first symptoms usually appear in people aged between 20 and 40 years. It is about twice as common in women as in men, and it mostly affects Caucasians living in temperate climates. MS may also run in families: a person is more likely to develop the disease if they have a parent or sibling with MS.
Diagnosis of multiple sclerosis
It can be challenging to diagnose MS, because the symptoms can be similar to other conditions and there is no one test to diagnose MS. Usually a person will have had at least 2 or more attacks of MS before it can be diagnosed.
If a general practitioner (GP) suspects MS based on a person’s symptoms, they will often refer them to a neurologist for further investigation. A neurologist will assess the person’s muscle strength and reflexes, and check for signs of muscle weakness, vision problems, difficulties with balance and coordination and speech problems.
The doctor may order tests including:
- Blood tests: Can help rule out other diseases that may have similar symptoms
- Magnetic resonance imaging (MRI) scan: Can show damage or scarring of the myelin sheath in the nerves of the brain and spinal cord
- Lumbar puncture (spinal tap): A small sample of fluid is removed from the spinal canal to check for antibodies associated with MS; can also identify signs of infection caused by other conditions
- Evoked potential tests: Examines the electrical signals produced by the nervous system and how quickly they pass through the system.
How does MS progress?
MS is an unpredictable disease. There is no way of knowing how the disease will progress in any particular person, or how mild or severe it will be. Just as the symptoms vary among individuals with MS, so does the course of the disease. Some people can be minimally affected, while others suffer severe progressive disability. However, the majority of people with MS do not become severely disabled.
In general, the course of MS tends to follow one of 2 patterns:
Relapsing-remitting MS: Most people have a form of relapsing-remitting MS, where the symptoms flare up (relapse) over several days or weeks and then settle down partially or completely (remission). Sometimes a person will be in remission for months or even years before another flare-up. Eventually, many people with relapsing-remitting MS will have a gradual progression of symptoms without periods of remission. This is called secondary-progressive MS.
Primary-progressive MS: Some people with MS have a steady worsening (progression) of symptoms without any relapses.
MS treatment
There is currently no cure for MS, but there are treatments available to treat MS attacks, change the course of the underlying disease and manage symptoms.
Treatment for an MS attack (relapse)
Steroid medicines – either given as tablets or injections – can help to shorten and reduce the severity of an MS attack. These medicines work by reducing inflammation and suppressing the immune system. They are only given for a few days at a time to minimise the risk of side effects.
Treatments to modify the course of MS
Medicines called ‘disease modifying therapies’ may be used to help reduce the number and severity of relapses. These medicines can reduce the damage to the myelin sheath that happens during a relapse. They can only be prescribed if the person meets certain criteria, as assessed by a doctor.
Disease modifying therapy includes medicines that specifically target the immune process in MS.
Immunomodulators
Immunomodulators can reduce the frequency of attacks and slow down the progress of MS. However, these treatments do not reverse current symptoms and there can be significant side effects with some medicines. Having a relapse while taking immunomodulators does not mean that the treatment isn’t helping.
Examples include the following.
- Interferon beta-1a (brand names Avonex and Rebif) and interferon beta-1b (Betaferon). Interferons are proteins produced naturally in the body that help to fight infections and regulate the immune system. Beta interferons have been shown to slow down the progress of MS by regulating the immune system, as well as reduce the frequency and severity of attacks. They are given by injection.
- Glatiramer acetate (brand name Copaxone) has similar effectiveness to interferon beta and is given by injection.
- Natalizumab (brand name Tysabri). This is a type of antibody that targets certain immune cells, stopping them moving from your bloodstream to the brain. It is given by intravenous infusion (through a drip into a vein). Natalizumab may increase the risk of a rare but very serious brain infection called progressive multifocal leucoencephalopathy, so your doctor may wish to monitor you for any signs of this.
- Alemtuzumab (Lemtrada) is also given through a drip into a vein and helps reduce the relapse rate in MS.
- Fingolimod (brand name Gilenya). This is an immunomodulator that targets the immune cells involved in destroying myelin. It helps trap them in the lymph nodes, reducing the number that can reach the brain and spinal cord. Fingolimod is given as a tablet.
- Dimethyl fumarate (Tecfidera) and teriflunomide (Aubagio) are also given as tablets.
Immunosuppressants
Immunosuppressants are another group of medicines that have a broader effect in dampening down the immune system than the immunomodulators. Your specialist may offer an immunosuppressant for progressive MS, or for relapsing-remitting MS if it does not respond to immunomodulators.
Treatments to relieve symptoms
Medicines may help to relieve muscle spasms and stiffness. Other medicines are available that can help to relieve pain, bowel and bladder control problems, fatigue and depression.
Physiotherapy and occupational therapy may also help you manage symptoms of MS and stay active.
Medical professionals who can help with MS
Several different medical professionals may be involved in caring for the person with MS. They include:
- Neurologists: specialists in treating conditions of the nervous system. It is generally a neurologist who makes the initial diagnosis of MS.
- Physiotherapists: help with exercise programs, strength and mobility.
- Speech therapists: help with speech and swallowing problems.
- Occupational therapists: help with managing daily activities and the need for aids or modifications around the house.
- Neuropsychologists: help with strategies to improve memory and thinking skills.
- Ophthalmologists: help with eye problems.
- General practitioners: help with monitoring overall health, medications and referrals to specialists.
- MS nurses: work in major hospitals and for state offices of MS Australia.
- Social workers: provide community support and home visits.
Living with MS
While MS may be challenging at times, with the right treatment and support, people with MS can lead long and healthy lives. Healthcare providers can provide valuable advice and education about MS, and discuss the treatment options that are best suited for each person. They can also help the person with MS to learn to care for themselves with lifestyle changes. Support groups are available around Australia for people with MS and their carers.