
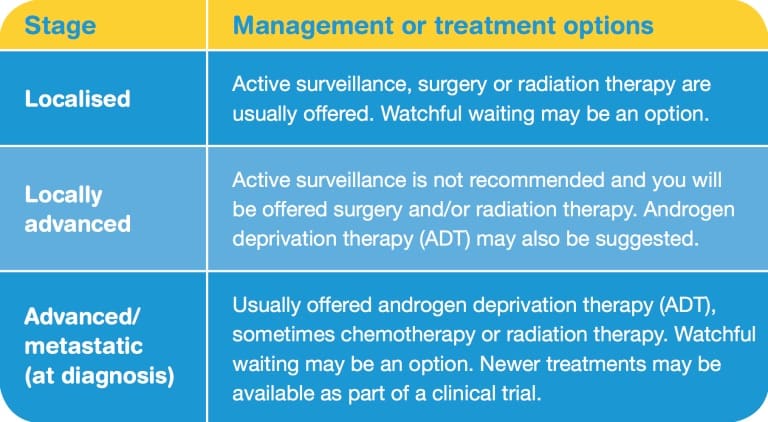
There are different options for managing and treating prostate cancer. For some men, immediate treatment is not necessary or may not be appropriate. Your treating specialist will let you know your options based on the stage and grade of the prostate cancer, as well as your general health, age and preferences.
Active surveillance
Active surveillance is a way of monitoring prostate cancer that isn’t causing any symptoms or problems. It may be suggested if the cancer is small (low volume) and slow-growing (low grade), and is unlikely to spread or cause symptoms (low risk or, in some cases, intermediate risk). This is indicated by a PSA no higher than 20, stage T1–2, and Grade Group score 1 (Gleason 6 or less). About half of all Australian men with low-risk prostate cancer choose active surveillance.
Typically, active surveillance involves:
- PSA tests every 3–6 months
- digital rectal examination every six months
- mpMRI scans, and biopsies at 12 months and three years.
If the cancer shows signs of faster or more aggressive growth, you can start treatment with the aim of curing the cancer.
Watchful waiting
Watchful waiting is another way of monitoring prostate cancer. This involves regular PSA tests and clinic check-ups. The monitoring process is less strict than for active surveillance, and further biopsies are usually not required. Treatment can be considered if the cancer spreads and/or causes symptoms. The aim of treatment will be to treat symptoms that may be causing problems, rather than cure the prostate cancer.
Watchful waiting may be suitable for older men where the cancer is unlikely to cause a problem in their lifetime. Some men choose watchful waiting instead of immediate cancer treatment if the cancer is already advanced. It can also be an option for men with other health problems that would make it hard to handle treatments such as surgery or radiation therapy.
Choosing active surveillance or watchful waiting avoids treatment side effects, but some men have ongoing anxiety about the cancer. Before deciding not to have treatment, think about ways to manage any worries. Talk to your doctors, or call Cancer Council 13 11 20.
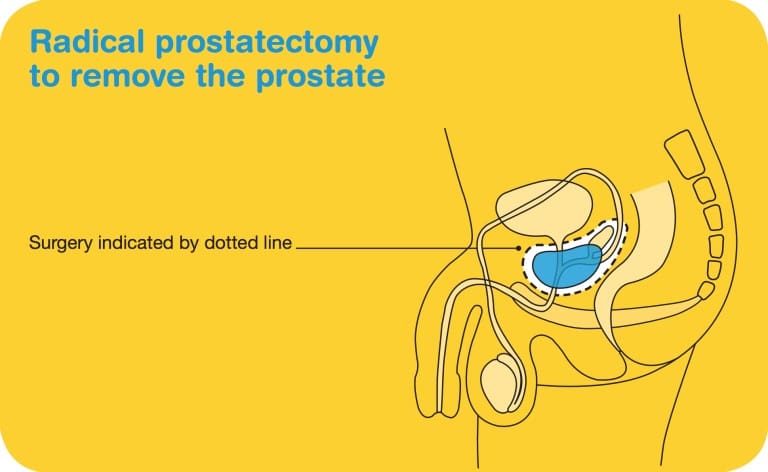
Surgery
Your doctor may suggest a radical prostatectomy if you have early prostate cancer and are fit enough for surgery. This operation aims to remove the cancer completely by removing the prostate, part of the urethra, and the seminal vesicles. For more aggressive cancer, nearby lymph glands may also be removed (pelvic lymph node dissection). After the prostate is removed, the urethra will be rejoined to the bladder and the vas deferens will be sealed.
For general information about surgery for cancer, see Cancer Council’s booklet Understanding Surgery. Call 13 11 20 for a free copy or look for it on your local Cancer Council website. The Prostate Cancer Foundation of Australia also has many useful resources, including Understanding Surgery for Prostate Cancer. Visit prostate.org.au or call 1800 22 00 99.
Types of radical prostatectomy
Radical prostatectomy may be performed using different surgical techniques. There may be extra costs involved for some options and they are not all available at every hospital.
Open radical prostatectomy
This is usually done through a cut in the lower abdomen.
Laparoscopic radical prostatectomy
Sometimes the prostate can be removed via keyhole surgery (also called laparoscopic surgery). Small surgical instruments are inserted through several small cuts in the abdomen, and the surgeon performs the procedure by moving the instruments while watching a screen.
Robotic-assisted radical prostatectomy
Laparoscopic surgery can be performed using a robotic device, which allows the surgeon to see a three-dimensional picture and to use more advanced instruments than those used for conventional laparoscopic surgery. This is called robotic-assisted laparoscopic radical prostatectomy or RARP.
Nerve-sparing radical prostatectomy
This involves removing the prostate and seminal vesicles and trying to preserve the nerves that control erections. This procedure is more suitable for lower grade cancers and is only possible if the cancer is not
in or close to these nerves. It is best performed on younger men who have good erectile function. Problems with erections are common even if nerve-sparing surgery is performed, but these can be managed (see pages 47−49).
Making decisions about surgery
Talk to your surgeon about what types of surgery are available to you. Ask about the advantages and disadvantages of each option, and if you will have any out-of-pocket costs.
The surgeon’s experience is more important than the type of surgery offered. Compared to open surgery, both standard laparoscopic surgery and robotic-assisted surgery usually mean a shorter hospital stay, less bleeding, a smaller scar and a faster recovery. However, there is currently no good, long-term evidence that one approach causes fewer ongoing side effects or better cancer outcomes.
Whichever surgical approach is used, a radical prostatectomy is major surgery and requires time to recover.
Side effects of prostate cancer surgery
You can expect to return to usual activities 4–6 weeks after surgery for prostate cancer. Most men can start driving again within a couple of weeks, but heavy lifting should be avoided for six weeks. You may experience some or all of the following side effects:
Nerve damage
The nerves needed for erections and the sphincter muscle required for bladder control are both close to the prostate. It may be very difficult to avoid these during surgery, and any damage can cause problems with erections and bladder control.
Loss of bladder control
You may have some trouble controlling your bladder after a radical prostatectomy. This condition is known
Management and treatment 31
as urinary incontinence. It usually improves a few months to a year after the surgery. A small number of men (about 5%) may be left with ongoing incontinence, which could need a further operation to fix. In rare cases, the incontinence may be permanent.
There are various ways to manage these problems, so it is worth seeing a continence physiotherapist or continence nurse before the surgery, or soon afterwards. In particular, pelvic floor exercises can help improve bladder control.
Erection problems (impotence)
Many men experience problems getting and keeping erections after prostate surgery.
It may take some months to a few years for erections to improve. Some men may not get strong erections again. Oral medicines, vacuum erection devices, injection therapy or implants may help if you have ongoing problems with erections (see pages 47–49).
Infertility
During a prostatectomy, the tubes from the testicles (vas deferens) are sealed and the prostate and seminal vesicles are removed, so semen is no longer ejaculated during orgasm. This is known as a dry orgasm and results in infertility (see pages 50–51). If having children is important to you, talk to your doctor before treatment about sperm banking or other options.
Penile shortening
In some men, the penis gradually becomes shorter after surgery. Regularly using a vacuum erection device (see page 48) can help maintain penis length. You can see a psychologist or counsellor for assistance coming to terms with any changes to the appearance of your penis.
Radiation therapy
Radiation therapy (also known as radiotherapy) is one of the treatments offered to men with early prostate cancer. It is generally offered as an alternative to surgery and has similar rates of success. It may also be offered if you are not well enough for surgery. Sometimes radiation therapy is used after a prostatectomy for locally advanced or more aggressive cancers, or if there are signs that not all of the cancer has been removed by surgery.
Radiation therapy can be delivered externally using external beam radiation therapy, or internally using brachytherapy. Most men who have radiation therapy as their initial treatment for more advanced prostate cancer will receive androgen deprivation therapy (ADT) beforehand and/or afterwards.
External beam radiotherapy (EBRT)
External beam radiation therapy (EBRT) uses targeted radiation to kill cancer cells or injure them so they cannot multiply. The radiation is usually in the form of x-ray beams.
Treatment is planned to ensure there is as little damage as possible to the normal tissue and organs surrounding the prostate. The planning sometimes involves inserting small pieces of gold (marker seeds) into the prostate to allow more accurate targeting of the radiation. This is called image-guided radiation therapy (IGRT).
Usually, EBRT for prostate cancer is given every weekday for up to eight weeks, often in combination with temporary androgen deprivation therapy (ADT).
Proton therapy for prostate cancer
A special type of EBRT uses protons rather than x-rays. This is known as proton therapy and is useful when the cancer is near sensitive areas, such as the brainstem and spinal cord. It is not yet available in Australia, but has been used in the US to treat prostate cancer. At this stage, there is no evidence that proton therapy provides better outcomes for prostate cancer than standard radiation therapy with x-rays.
Each EBRT treatment session takes about 15 minutes. You will lie on the treatment table under the radiation machine. The machine does not touch you but may rotate around you. You will not see or feel the radiation. EBRT does not make you radioactive and there is no danger to the people around you.
Side effects of EBRT
You may experience some of the following side effects. Most will be temporary and there are ways to manage them.
Erection problems (impotence)
EBRT can damage the nerves that control erections. This can make it hard to get and keep an erection, especially in men who already had trouble with erections because of their age. ADT can make the problem worse. This side effect does not always occur immediately, but may develop over time and be ongoing.
Changes in ejaculation
Some men notice pain on ejaculation or find that they ejaculate less or not at all (dry orgasm) after. The discomfort usually eases over time, but dry orgasms may be a permanent side effect.
Infertility
Radiation therapy to the prostate usually results in infertility. If you wish to have children, speak to your doctor before treatment about sperm banking or other options.
Skin irritation
Skin in the area treated may become red and sore (like mild sunburn) during or soon after treatment. These reactions fade with time. Ask your treatment team for advice.
Tiredness
You may become very tired because your body is coping with the effects of radiation on normal cells. Fatigue may build up slowly during treatment and should go away afterwards, but can last up to six months. Talk to your radiation oncologist or call Cancer Council 13 11 20 to find out about programs that can help improve fatigue after cancer treatment.
Urinary problems
You may experience a burning sensation when urinating, or an increased urgency to urinate. These side effects usually go away after treatment, but your doctor can prescribe medicine to reduce any discomfort. Radiation is unlikely to cause incontinence, but it can damage the lining of the bladder. In rare cases, this can lead to ongoing bleeding (radiation cystitis), which can be difficult to control. Let your doctor know of any problems with urinating or bleeding.
Bowel problems
It is common to have a feeling of being unable to completely empty the bowel and/or to develop haemorrhoids. Management and treatment 35 Less commonly, men may bleed when passing a bowel motion. This is caused by damage to the fine blood vessels in the lower bowel. Tell your doctor if you have any bleeding from the rectum. Some men may also have diarrhoea or difficulty holding onto their bowel motions. These side effects usually go away in time.
Brachytherapy
Brachytherapy is a type of targeted internal radiation therapy where the radiation source is placed directly within the prostate. This allows doses of radiation to be given directly inside of the prostate, and limits the effects on nearby tissues such as the rectum and bladder. Brachytherapy can be given by inserting permanent “seeds” that are radioactive for a few months, or through temporary needle implants. Brachytherapy is not suitable for men who already have significant urinary symptoms, or a very small or very large prostate gland.
Permanent brachytherapy
This treatment is most suitable for men with a small to medium sized prostate, few urinary symptoms, and small tumours with a low PSA level (less than 10) and a low/intermediate Grade Group or Gleason score. It can sometimes be an expensive treatment option, so check what costs are involved before making a decision.
Permanent brachytherapy involves putting radioactive seeds, about the size of an uncooked grain of rice, into the prostate. It is also called low-dose-rate (LDR) brachytherapy. The seeds are 36 Cancer Council inserted under a general anaesthetic through the skin between the scrotum and anus using needles. They are guided into place with the help of an ultrasound. There is no incision, only some small puncture holes that heal very quickly, allowing for a faster recovery than EBRT or surgery. The procedure takes only 1–2 hours and you can usually go home the same day.
The seeds slowly release radiation to kill cancer cells, and lose their radioactivity after about three months. They are not removed from the prostate.
The level of radiation that comes from the seeds is low, but you will need to take care around pregnant women and young children for several weeks – your treatment team will explain the precautions to you. Although very uncommon, it is possible that a seed may dislodge during sexual activity. For this reason, you will be advised to use a condom or avoid sexual activity for three months. This way if a seed comes out, the condom will catch it.
Temporary brachytherapy
Also known as high-dose-rate (HDR) brachytherapy, temporary brachytherapy may be offered to men with higher PSA levels and Grade Group scores who are at risk of locally advanced cancer. It is often given with a short course of EBRT.
In temporary brachytherapy, the radiation is delivered through hollow needles that are inserted into the prostate, usually under general anaesthetic. These needle implants stay in place for several hours. During this time, you will have three brachytherapy sessions. For each session, radioactive wires will be inserted into the needles to deliver a high dose of radiation for about a minute. Once the wires are removed after each session, you will not be radioactive and there is no risk to other people. You will need to stay in hospital overnight for this treatment, and the needle implants will be removed before you go home.
Side effects of brachytherapy
The side effects of brachytherapy usually start 1–2 weeks after treatment and start to resolve within a couple of months. They may include pain when urinating, blood in the urine, poor urine flow and bladder irritation. Permanent radioactive seeds have the lowest chance of causing erection problems compared with other treatments. Erection problems and changes in ejaculation (such as pain or dry orgasm) sometimes occur after temporary needle implants. Talk to your doctor and/or treatment team about ways to manage these side effects. See pages 46–57 for more information
More information about radiation therapy
To find out more about radiation therapy, call Cancer Council 13 11 20 for a free copy of Understanding Radiation Therapy, or visit your local Cancer Council website. The Prostate Cancer Foundation of Australia have a resource called Understanding Brachytherapy for Prostate Cancer − visit prostate.org.au or call 1800 22 00 99. You can also visit targetingcancer.com.au for more information and videos explaining radiation therapy.
Androgen deprivation therapy (ADT)
Prostate cancer needs testosterone to grow. Slowing the production of testosterone may slow the growth of the cancer or shrink it temporarily. Testosterone is an androgen (male sex hormone), so this treatment is called androgen deprivation therapy (ADT). It is also known as hormone therapy.
ADT injections
The most common form of ADT involves injections of drugs that block the body’s production of testosterone. They are usually given monthly, four-monthly or six-monthly. These injections will not cure the cancer but may slow its growth for years.
ADT injections are often used before, during and after radiation therapy. They are the main treatment for advanced prostate cancer, often combined with chemotherapy.
Intermittent ADT
Occasionally ADT injections may be given in cycles, with treatment continuing until your PSA level is low, and then stopped for a period of time. It can then be restarted if your PSA rises again. This is known as intermittent ADT. In some cases, this can reduce side effects without affecting long-term prostate cancer outcomes. However, it is not suitable for all men.
Anti-androgen tablets
Often just called hormone tablets, anti-androgen tablets are taken by mouth. While ADT injections work by blocking the body’s production of testosterone, anti-androgen tablets stop the testosterone reaching the cancer cells. Anti-androgen tablets 40 Cancer Council are sometimes used on their own. More often, they are used with ADT injections. This combination is known as a complete or combined androgen blockade.
Surgical approach
Removing all or part of the testicles permanently reduces testosterone levels. This surgical approach is no longer commonly used, but some men with advanced prostate cancer may still prefer it over regular injections or tablets.
The removal of both testicles is called a bilateral orchidectomy. Some men have a silicone prosthesis put into the scrotum after surgery to keep its shape. The removal of only the inner part of the testicles (subcapsular orchidectomy) does not need a prosthesis.
Side effects of ADT
ADT may cause a range of side effects because of the reduced testosterone levels in the body. These can include:
- fatigue
- reduced sex drive (libido)
- erection problems
- loss of muscle strength, weight gain
- hot flushes, breast growth and tenderness
- mood swings, depression, trouble with thinking and memory
- loss of bone density (osteoporosis) – your doctor may monitor your bone mineral density, calcium and vitamin D levels
- increased risk of other problems such as obesity, diabetes and heart disease – your doctor will assess these risks with you and it may be helpful to seek advice from a dietitian.
Although the side effects of ADT can be significant, your treatment team can help you minimise the impact. To read more about this treatment, see Understanding Hormone Therapy for Prostate Cancer, available from the Prostate Cancer Foundation of Australia. Visit prostate.org.au or call 1800 22 00 99
Advanced prostate cancer treatment
ADT is the main treatment for advanced prostate cancer, when disease has spread beyond the prostate. In this case, the treatment will not cure the cancer but can keep it under control for months and even years. It may also reduce or eliminate the symptoms of cancer (temporary remission) and help with symptoms such as pain caused by the cancer spreading.
Chemotherapy (see below) and external beam radiation therapy are also standard treatment options for advanced prostate cancer. These may be offered in combination with ADT.
Chemotherapy
Chemotherapy is the use of drugs to kill or slow the growth of cancer cells. If the prostate cancer continues to advance and spread to other parts of your body despite using ADT, chemotherapy may be suitable. Chemotherapy may also be offered as your first treatment in combination with ADT.
Generally, chemotherapy is given through a drip (infusion) into a vein (intravenously). It is usually given once every three weeks and you do not need to stay overnight in hospital.
To find out more about chemotherapy, call Cancer Council 13 11 20 and ask for a free copy of Understanding Chemotherapy, or visit your local Cancer Council website.
Side effects of chemotherapy may include fatigue; hair loss; changes in blood counts increasing the risk of bleeding or infections; numbness or tingling in the hands or feet (peripheral neuropathy); changes in nails; and rare side effects, such as allergic reactions or blockages of the tear ducts. Fortunately, improved medicines have greatly reduced the impact of chemotherapy on quality of life.
Transurethral resection of the prostate (TURP)
TURP is a surgical procedure to relieve blockages in the urinary tract. It helps with symptoms of more advanced prostate cancer, such as frequent urination, but does not cure the cancer. TURP is also used to treat benign prostate hyperplasia.
You will be given a general or a spinal anaesthetic. A small telescope-like instrument is passed through the opening of the penis and up the urethra to remove the blockage. The surgery takes about an hour, and you will usually need to stay in hospital for a couple of days.
Bone therapies
If you have prostate cancer that has spread to the bones, your doctor may suggest treatments to manage the impact on the bones. Drugs can be used to prevent or minimise bone pain and can reduce the risk of fractures and compression on the spinal cord. Radiation therapy can also be used to reduce bone pain, or to prevent or assist in the repair of fractures or spinal cord compression.
Other therapies
Newer drug therapies may be used to treat men with advanced prostate cancer that has stopped responding to ADT. This is known as second-line treatment. These drugs, such as abiraterone and enzalutamide, are hormone tablets that can be combined with ADT to help prolong life and reduce symptoms. Clinical trials are investigating whether these newer drugs should be given when ADT is started for advanced prostate cancer (first-line treatment).
Palliative treatment
Palliative treatment aims to improve quality of life by reducing cancer symptoms without trying to cure the disease. It can be used for symptom control at different stages of cancer, not just at the end of life. Palliative treatment is particularly important for people with advanced cancer. It can assist with managing symptoms such as pain, and slow the spread of the cancer.
Palliative radiation therapy may be used to treat pain, such as bone pain if the cancer has spread to the bones (bone metastases). Pain-relieving medicines (analgesics) are also often used.
Call Cancer Council 13 11 20 for free copies of Living with Advanced Cancer, Understanding Palliative Care or Overcoming Cancer Pain, or visit your local Cancer Council website.
Making treatment decisions
Prostate cancer is typically slow-growing, giving men time to make decisions about their management or treatment options.
Sometimes it is difficult to decide on the type of management or treatment that is right for you. You may feel that everything is happening too fast. Check with your doctor how soon you need to make a decision and take as much time as you can. Understanding the disease, treatment options and possible side effects can help you make an informed decision that’s based on your personal values.
If you are offered a choice of management or treatment, you will need to:
- weigh up the pros and cons
- consider how important any possible side effects are to you
- think about the cost and availability of treatment (some treatments, such as brachytherapy and robotic-assisted surgery, are only available in some locations and may cost more).
If you have a partner, you may want to talk about treatment options with them. You can also talk to friends and family or men you know who have had prostate cancer. If only one type of treatment is recommended, ask your doctor to explain why other treatment choices have not been offered. You also have the right to accept or refuse any treatment offered.
Some men with more advanced prostate cancer may choose treatment even if it only offers a small benefit for a short period of time. Such options often won’t cure the cancer but may slow its progress and improve quality of life.
Talking with doctors
When your doctor first tells you that you have cancer, you may not remember the details about what you are told. Taking notes or recording the discussion may help. Many people like to have a family member or friend go with them to take part in the discussion, take notes or simply listen.
If you are confused or want clarification, you can ask questions, scroll to end of this article for a list of suggested questions. If you have several questions, you may want to talk to a nurse, such as a prostate cancer specialist nurse or cancer care coordinator, or ask the office manager if it is possible to book a longer appointment.
A second opinion
You may want to get a second opinion from another specialist to confirm or clarify your doctor’s recommendations or reassure you that you have explored all of your options. Specialists are used to people doing this.
Your doctor can refer you to another specialist and send your initial results to that person. You can get a second opinion even if you have started treatment or still want to be treated by your first doctor. You might decide you would prefer to be treated by the doctor who provided the second opinion.
Taking part in a clinical trial
Your doctor or nurse may suggest you take part in a clinical trial. Doctors run clinical trials to test new or modified treatments and ways of diagnosing disease to see if they are better than current methods. For example, if you join a randomised trial for a new treatment, you will be chosen at random to receive either the best existing treatment or the modified new treatment.
Over the years, trials have improved treatments and led to better outcomes for people diagnosed with cancer.
It may be helpful to talk to your specialist or clinical trials nurse, or get a second opinion. If you decide to take part, you can withdraw at any time. For more information, call Cancer Council 13 11 20 for a free copy of Understanding Clinical Trials and Research, or visit australiancancertrials.gov.au.
What if I am in a same-sex relationship?
It important to feel that your sexuality is respected when discussing how cancer treatment will affect you. Your medical team should be able to openly discuss your needs and support you through treatment. Try to find a doctor who helps you feel at ease talking about sexual issues and relationships.
If you have a partner, encourage him to come to medical appointments with you. This will show your doctor who’s important to you and will enable your partner to be included in discussions and treatment plans.
You can contact the Prostate Cancer Foundation of Australia (PCFA) on 1800 22 00 99 or at prostate.org.au to request a free copy of the Prostate Cancer Pack: Information for Gay and Bisexual Men. PCFA also have support group.
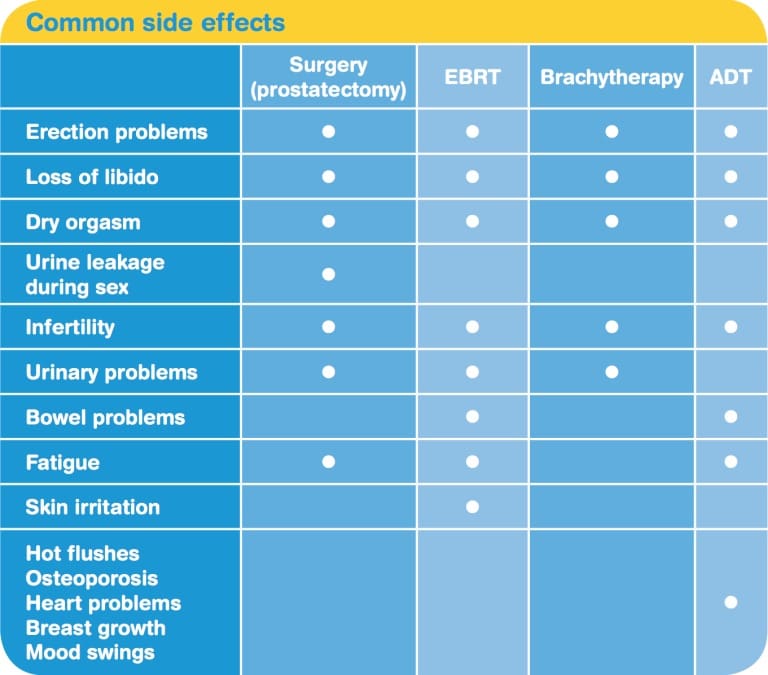
Managing side effects
Treatment for prostate cancer may cause a range of side effects, which will vary depending on the treatment and from person to person. Keep in mind that some men do not have any of the side effects listed below. When men do experience side effects, the changes often last for only a few weeks or months, although in some cases they will be permanent. Fortunately, there are many ways to reduce or manage side effects.
Erection problems
When a man has trouble getting or keeping an erection firm enough for intercourse or other sexual activity, it is called erectile dysfunction or impotence. The quality of erections usually declines naturally as men get older. It can also be affected by other factors, including health conditions such as diabetes and heart disease; certain medicines for blood pressure or depression; previous surgery to the bowel or abdomen; smoking or heavy drinking; or emotional or mental distress.
Erection problems are common in men after treatment for prostate cancer. The prostate lies close to nerves and blood vessels that are important for erectile function. These can be damaged during surgery or radiation therapy. There may be a gradual recovery, with some men noticing their erectile function continues to improve for up to three years after treatment has finished.
Before and after treatment, various methods can help preserve the health of the penis (penile rehabilitation). These may include:
- engaging in foreplay and other sexual intimacy with your partner
- encouraging erections, starting a month after surgery
- taking prescribed medicines to maintain blood flow in the penis
- using a vacuum erection device to stop the penis shortening or losing flexibility
- injections of medicine into the penis.
Read on for more detail about these methods and tips on managing changes to your sex life. For many men, an orgasm can still be achieved without a full erection.
Ways to improve erections
There are several medical options for trying to improve the quality of your erections, regardless of the type of prostate cancer treatment you have had. Ask your treatment team for more details about these methods.
Oral medicines
There are tablets available on prescription that can help the body’s natural response to sexual stimulation by increasing blood flow to the penis. These can only help with erections if the nerves are working, which is unlikely in the early stages of recovery. However, your doctor may recommend using the tablets before and soon after surgery, as the increased blood flow can help preserve penis health until the nerves recover.
Side effects may include nausea, headaches, facial flushing and backache, but these only last for a few hours after taking a tablet. The drugs can cause blood pressure changes and should not be taken with some heart medicines.
Vacuum erection device
A vacuum erection device (VED) or vacuum pump device uses suction to draw blood into the penis. This device can also help to strengthen or maintain a natural erection.
You place a rigid tube over the penis. A manual or battery-operated pump then creates a vacuum that forces blood to flow into the penis so it gets hard. A band at the base of the penis keeps the erection firm after the pump is removed, and can be worn comfortably for 30 minutes.
Injections
Penile injection therapy (PIT) has to be prescribed by a doctor.
You will be taught to inject the penis with medicine that makes blood vessels in the penis expand and fill with blood, causing an erection. The erection usually occurs within 15 minutes and lasts 30–60 minutes.
Most often, the syringes come pre-loaded with the medicine and are single use. The needle is very short and fine, and usually causes only a moment of discomfort.
This treatment works well for most men, but a few may have pain and scarring. A rare side effect is a prolonged and painful erection (priapism) – this requires emergency medical attention.
Implants
A penile prosthesis is an implant that is inserted into the penis during surgery under general anaesthetic. This implant allows you to mechanically create an erection. Flexible rods or thin, inflatable cylinders are placed in the penis and connected to a pump in the scrotum. The pump is turned on or squeezed when an erection is desired.
Penile implants can be expensive, so check costs with your doctor. They generally won’t be offered for at least a year after prostate cancer treatment, and less invasive options, such as oral medicines or injections, will usually be tried first. Implants can be effective, but part of the tissue within the penis is removed to implant the device. This is a permanent change to the structure of the penis and a man will be unable to achieve an erection if the device is removed.
You may see or hear ads offering treatment for erection problems. Products that are widely available include herbal preparations, natural therapies, nasal sprays and lozenges. Talk to your doctor before using any of these, as there could be risks without any benefits. Those that contain testosterone or act like testosterone in the body may encourage the prostate cancer to grow.
Other changes to sexuality
You may notice other changes to your sexual functioning, which can affect the way you experience sexuality and intimacy.
Loss of libido
Reduced interest in sex (low libido) is common during cancer treatment. Quite often it occurs due to anxiety and fatigue rather than the treatment itself. However, libido can also be affected by ADT, which lowers testosterone levels, and by the sexual side effects associated with radiation therapy or surgery.
Most men notice that their sex drive returns when treatment ends, but for some men, the problem is ongoing. Adjusting to changes in sex drive can be emotionally and physically challenging for men and their partners.
Dry orgasm
After a prostatectomy, you won’t produce semen, as the prostate and seminal vesicles have been removed and the vas deferens are sealed. You will still feel the muscular spasms and pleasure that accompany an orgasm, but you will not ejaculate. This is called a dry orgasm. Some men notice that their orgasms feel less intense. You may worry that a dry orgasm will be less pleasurable for your partner. However, most partners say this is not the case, especially as many do not feel the release of semen during intercourse. Semen production may also be reduced after radiation therapy.
Urine leakage during sex
Some men who have had a prostatectomy notice a small leakage of urine during intercourse and orgasm. This is due to damage to the sphincter muscle that controls urine flow.
Urine leakage during sex can be embarrassing, but is not harmful to your partner. If this is a problem for you, empty your bladder (urinate) before sex. You can use a condom or a constriction ring (available from sex shops) at the base of the penis during sex to prevent leakage. Speak with your doctor if you are still concerned.
Fertility problems
After surgery, radiation therapy or ADT for prostate cancer, most men become infertile. This means they can no longer father children naturally. If you may want to have children in the future, you and your partner should talk to your doctor about the options before treatment starts. You may be able to store some sperm at a fertility clinic for use at a later time when you are ready to start a family.
To find out more, call Cancer Council 13 11 20 and ask for a copy of Fertility and Cancer, or visit your local Cancer Council website.
Restoring your sex life
Whether you are single, in a relationship, heterosexual, gay, bisexual or transgender, cancer can affect your sexuality in both physical and emotional ways. The impact of these changes depends on many factors, such as the cancer treatment and its side effects, how you and your partner communicate, and your level of self-confidence.
The importance of sexual activity for a man before prostate cancer will influence how changes to his sex life affect him (and his partner, if he has one) after treatment. Some men link their sense of masculinity with their sex drive, making adjusting to changes difficult. Others might feel they have lost a part of themselves or may question their self-worth.
For many people, a relationship based on trust and understanding is an important part of a satisfying, intimate sexual experience.
Communicating with a new partner
Deciding when to tell a potential sexual partner about your cancer experience isn’t easy. Some single men may avoid dating for fear of rejection.
While the timing will be different for each person, it can be helpful to wait until you and your new partner have developed a mutual level of trust and caring. However, it is best to talk with a new partner about your concerns before becoming sexually intimate. By communicating openly, you avoid misunderstandings and may find that your partner is more accepting and supportive.
Managing changes in your sex life
- Talk about the changes and your feelings about sex. If you have a partner, these changes will probably affect you both. Reassure them that intimacy is still important to you. • Be intimate without having sexual intercourse. Other ways of expressing love include touching, holding, caressing and massage.
- Take time to get used to any changes. Look at yourself naked in the mirror and touch your genitals to feel any differences or soreness. Show your partner the changes so they can adjust to them.
- Take things slowly. Start by touching each other’s skin, then include genital touching.
- Attempt intercourse even with a partial erection. This stimulation may encourage further and better erections.
- Explore your ability to enjoy sex and understand any changes by masturbating.
- Ask your partner to be gentle, as the genital area may be tender. Use silicone-based lubricants for prolonged stimulation. Practise reaching orgasm through methods such as hand-stroking.
- Try different positions to find out what feels comfortable for both of you. Having sex while kneeling or standing may also help with erections.
- Talk to your doctor, a sexual health physician or counsellor if the changes are causing depression or problems in your relationship.
- Call Cancer Council 13 11 20 for a copy of our Sexuality, Intimacy and Cancer booklet, or find it on your local Cancer Council website.
- Read Understanding Sexual Issues Following Prostate Cancer Treatment from the Prostate Cancer Foundation of Australia (prostate.org.au or 1800 22 00 99).
Urinary problems
Trouble controlling the flow of urine (urinary incontinence) is a common side effect of treatment. It is usually temporary. After prostate surgery, most men have some degree of incontinence for 3–6 months. Some lose a few drops of urine when they cough, sneeze, strain or lift something heavy. For others, symptoms may be more severe and require the use of incontinence pads.
In rare cases, radiation therapy can reduce how much urine the bladder can store, irritate the bladder, narrow the urethra and weaken the pelvic floor muscles. This can lead to urinary urgency (feeling like you just can’t wait) and difficulty passing urine.
Other side effects
Treatment for prostate cancer may lead to a range of other concerns, but most of these can be managed.
Bowel problems
Although this is no longer a common side effect, radiation therapy can damage the rectum, leading to bleeding and/or diarrhoea. A bowel specialist such as a gastroenterologist or colorectal surgeon may treat these bowel problems with steroid suppositories (a tablet that you insert into the rectum through the anus) or other treatments applied to the bowel. For more information, talk to your radiation oncologist or a continence nurse. You may also want to read Understanding Bowel Disturbance Following Prostate Cancer Treatment, available from the Prostate Cancer Foundation of Australia (prostate.org.au or 1800 22 00 99).
Coping with urinary incontinence
- Find out about pelvic floor exercises. Men who do pelvic floor exercises before surgery are less likely to have ongoing urinary incontinence after surgery. The exercises are also important after surgery. Ask your doctor, urologist, physiotherapist or continence nurse for more information.
- Drink plenty of water to dilute your urine − concentrated urine can irritate the bladder. Avoid restricting your fluid intake because you are afraid of leakage. Dehydration can cause constipation, which can also lead to leakage.
- Limit tea, coffee, alcohol and carbonated drinks – these can all irritate the bladder.
- Talk to a continence nurse about continence aids if needed. These aids can include absorbent pads to wear in your underpants, and bed and chair covers. The nurse may also recommend medicines or special clamps.
- Ask your continence nurse or GP about the Continence Aids Payment Scheme. This assists men who have ongoing incontinence with the cost of continence products.
- If incontinence hasn’t improved after 12 months, talk to your doctor or urologist about whether surgical treatment is an option. For example, a surgically inserted sling or artificial sphincter works by putting pressure on the urethra to close it off and control urinary flow.
- Call 13 11 20 or visit your local Cancer Council website for a copy of Exercise for People Living with Cancer. This includes information on pelvic floor exercises.
- Get more resources from the Prostate Cancer Foundation of Australia (1800 22 00 99 or prostate.org.au) and the Continence Foundation of Australia (1800 33 00 66 or continence.org.au).
Fatigue
Cancer treatment often makes people very tired. After surgery, it may take some time to get back strength. With external beam radiation therapy, you may get particularly tired near the end of treatment and for some weeks or months afterwards. Regular exercise can help to reduce tiredness. Call Cancer Council 13 11 20 to find out about programs that can help. You can also request a copy of Exercise for People Living with Cancer, or find it on your local Cancer Council website.
Skin irritation
External beam radiation therapy can make the skin in the genital area red and sore for a time. Follow skin care instructions from your treatment team, even before you notice skin changes. Check with your treatment team before using any over-the-counter creams.
Hot flushes
You may experience hot flushes if you are having ADT. Reducing alcohol intake, avoiding hot drinks, getting regular exercise and learning relaxation may help.
Osteoporosis
Osteoporosis can be a delayed side effect of ADT, so your GP may need to monitor your bone mineral density.
Heart problems
Because ADT can lead to heart problems and strokes, your GP or specialist will monitor your heart function and may refer you to a dietitian or exercise physiologist for advice.
Other ADT side effects
Weight gain, mood swings, enlarged breasts, decreased muscle mass, change in body shape, and high cholesterol may be associated with prolonged use of ADT.
Key points
- Prostate cancer treatment may damage nerves and muscles near the prostate, bladder and bowel.
- Side effects may include erection problems, urinary incontinence, a lowered sex drive and infertility. These vary from person to person.
- It is common for men with prostate cancer to have problems getting and maintaining an erection.
- You may be able to improve the quality of your erections by taking tablets, using a vacuum erection device, giving yourself injections or getting an implant.
- You may have a reduced interest in sex (lowered libido). Most men notice that their sex drive returns when treatment finishes, but for some men this side effect is ongoing.
- If your semen production is reduced, you will have dry orgasms. This means you will feel the pleasurable sensation of an orgasm, but semen will not come out of the penis (ejaculation).
- Most men become infertile after treatment for prostate cancer. If you want to have children, talk to your doctor about options such as sperm storage before the cancer treatment starts.
- Urinary incontinence is trouble controlling the flow of urine. It may be worse soon after treatment and improve over time. A continence nurse or a continence physiotherapist can help. Surgery may be an option.
- Taking time to adjust and getting support from your partner and medical team may help you cope with side effects.